Introduction
Atopic dermatitis (AD), commonly referred to as eczema, is a chronic inflammatory skin condition that predominantly begins in early childhood. This chapter is designed to provide a comprehensive understanding of AD, tailored to the needs of pharmacy students preparing for the PEBC exams in Canada. By focusing on the clinical presentation, associated conditions, therapeutic goals, and key diagnostic considerations, this chapter aims to equip future pharmacists with the knowledge to support patients effectively.
Atopic dermatitis manifests as episodes of dermatitis characterized by poorly defined areas of erythema, scaling, and excoriations. In more chronic cases, patients may present with lichenification, a hallmark feature involving thickened skin and pronounced skin markings due to prolonged rubbing. The condition is often accompanied by intense itching (pruritus) and generalized dry skin, which can significantly impact the quality of life.
While some children may outgrow the condition, a subset of patients will continue to experience symptoms well into adulthood. AD frequently coexists with other atopic disorders such as asthma, allergic rhinoconjunctivitis, and food allergies, highlighting its role in the broader atopic disease spectrum.Goals of Therapy for Atopic Dermatitis
Since atopic dermatitis is a chronic and relapsing condition with no definitive cure, management revolves around symptom control. The primary goals of therapy include:
Managing Dry Skin and Pruritus: Relieving widespread dryness and itching, especially when these symptoms interfere with daily life.
Treating Dermatitis Lesions: Addressing inflammation and pruritus in active dermatitis patches to minimize discomfort and lower the risk of secondary bacterial infections.
Preventing Flare-Ups: Identifying and mitigating triggers such as environmental irritants that can exacerbate the condition.
Prompt Treatment of Complications: Managing complications like:
Secondary bacterial infections (e.g., impetigo, often caused by Staphylococcus aureus).
Viral infections (e.g., eczema herpeticum, caused by the herpes simplex virus).
Clinical Presentation and Diagnostic Considerations
Morphological Patterns by Age Group:
Infants: The rash typically appears on the face and extensor surfaces of the limbs.
Older Children: Flexural areas such as the elbows and knees are commonly affected.
Adults: The dermatitis often becomes prominent on the face and hands.
The variability in presentation across age groups underscores the importance of tailoring treatment to the individual.
Although routine diagnostic tests are not usually necessary for classical AD, in cases where treatment-resistant lesions are observed, Bacterial Culture Swabs is used to identify secondary infections in persistent patches. Moderate to heavy growth of organisms may indicate bacterial superinfection, although interpreting minimal growth is challenging since many patients with AD are colonized with Staphylococcus aureus.
Therapeutic Choices in Atopic Dermatitis Management
Prevention
Moisturizer Application in Infants at Risk: Early studies suggested that daily application of moisturizers to infants with a high risk of developing atopic dermatitis (AD) might reduce the likelihood of the condition. However, larger follow-up studies failed to confirm these findings, and the preventive role of moisturizers remains unproven.
Probiotics During Pregnancy and Breastfeeding:
Maternal use of probiotics during pregnancy and breastfeeding, as well as direct administration to infants, may help reduce the risk of developing AD in children, particularly in high-risk families (e.g., mothers with other children affected by AD).
Most studies used strains of Lactobacillus, but there is no consensus on the specific strain, dose, or duration of use due to inconsistent study results.
Current evidence indicates probiotics may be considered for high-risk mothers, but further safety data are needed to confirm their efficacy and risks.
Dietary Restrictions During Pregnancy/Breastfeeding:
Evidence does not support advising women to avoid specific foods during pregnancy or breastfeeding to prevent allergic diseases like AD in their children.
Nonpharmacologic Choices
Patient Education:
Formal, disease-specific education programs significantly enhance treatment outcomes for both children and adults with AD.
Avoidance of Environmental Irritants:
Reducing exposure to common irritants, such as perfumed products, wool, harsh soaps, dry grass, and leaves, is beneficial.
Identifying and minimizing individual triggers (e.g., stress, allergens) can prevent flares. For stress-induced flares, focus on effective stress management strategies.
Dietary Interventions:
Food ingestion as a cause of AD flares is uncommon.
Elimination diets, such as removing cow's milk, have not shown consistent benefits in managing AD.
For patients with suspected egg allergies, avoiding eggs may help, but further research is required to confirm this benefit.
Bathing and Skin Care:
While bathing is often considered integral to AD care, evidence does not strongly support its necessity for improving the skin condition.
Recommendations for bathing include:
Keeping baths brief (5–10 minutes) and using warm, not hot, water.
Patting the skin dry and applying moisturizer within 3 minutes to lock in moisture.
Adding emollients or oils to bathwater does not offer additional benefits and may increase the risk of slipping.
Wet Wrap Therapy:
Wet wraps (bandages applied over moisturizers or medications) may provide second-line relief, though evidence is limited and of poor quality. They should only be used under physician supervision due to risks like infection, tissue maceration, or excessive medication absorption.
Dry-Wrap Therapy:
Occlusion with dry-wrap therapy or similar methods is unnecessary as appropriate topical therapy achieves lesion healing effectively.
Pharmacologic Choices
Moisturizers:
Moisturizers are a cornerstone of AD treatment, helping to restore skin hydration and prevent flares.
Key considerations for selecting and using moisturizers include:
Applying them liberally at least once daily or more frequently if needed.
Choosing fragrance-free, nonirritating products.
Ensuring the product is affordable and suited to patient preferences (e.g., texture, smell).
During puberty, using noncomedogenic moisturizers on the face to avoid acne.
Petroleum jelly is a cost-effective and highly effective option for many patients.
Topical Corticosteroids:
These are first-line pharmacologic agents for controlling inflammation and itching in AD.
The potency of corticosteroids depends on factors such as molecular structure, vehicle, and skin integrity. Treatment should:
Match the corticosteroid potency and vehicle to the lesion severity and location.
Continue until the rash and itching resolve, typically a few days to weeks.
Avoid common pitfalls like inadequate application or insufficient quantities, which often lead to suboptimal results.
The concept of Fingertip Units (FTUs) helps guide the correct application of corticosteroids:
One FTU (approximately 0.5 g) covers an area of 250 cm², equal to two adult handprints.
Table 3 provides specific FTU recommendations based on patient age and body site.
"Steroid-phobia," or fear of corticosteroid side effects, often results in undertreatment, exacerbating AD symptoms and complications like secondary infections and sleep disturbances. Patient education is essential to combat misconceptions and promote adherence.
Table 1: Recommended Corticosteroid Potency Based on Body Area
Table 2: Characteristics of Topical Corticosteroid Vehicles
Table 3: Fingertip Unit (FTU) Estimates for Topical Corticosteroid Application by Body Area
Calcineurin Inhibitors and Topical Immune Modulators
Calcineurin inhibitors, such as tacrolimus and pimecrolimus, are effective topical medications designed to inhibit calcineurin, providing targeted anti-inflammatory effects compared to the broader actions of corticosteroids. These agents are available in Canada and are approved as second-line therapies for both short- and long-term intermittent use in managing atopic dermatitis (AD). They are sometimes used off-label as first-line treatment, particularly for sensitive areas like the face or intertriginous folds, where frequent use of corticosteroids raises concerns.
Tacrolimus ointment has been found to be slightly more effective than pimecrolimus cream, though practical considerations such as the formulation type (ointment vs. cream) often influence treatment decisions. Calcineurin inhibitors typically require twice-daily application and work slower than corticosteroids. They can be used alongside corticosteroids applied to other body areas, though combining these agents with topical corticosteroids does not show additional benefits.
Phosphodiesterase-4 Inhibitors
Crisaborole, a phosphodiesterase-4 inhibitor, is a newer topical anti-inflammatory approved for mild to moderate AD on all body areas. Early studies indicate it can improve AD and associated pruritus, though its place in therapy relative to other treatments remains under evaluation.
Barrier Repair Therapies
Barrier repair products aim to address the defective skin barrier observed in AD by restoring ceramide balance. Some studies suggest ceramide-dominant products are as effective as mid-potency corticosteroids over a 28-day period, while others report no significant advantage compared to standard moisturizers or other barrier repair therapies.
Probiotics and Dietary Supplements
Evidence for probiotics in the treatment of established AD remains conflicting, but studies have not reported increased risks of adverse events. Regarding dietary supplements, there is no robust evidence supporting the effectiveness of vitamin D, selenium, fish oil, or zinc in treating AD. Similarly, herbal products like borage oil or evening primrose oil lack efficacy for AD management.
Advanced and Systemic Therapies
Patients with extensive, severe, or refractory AD may benefit from systemic treatments or advanced therapies such as:
Systemic agents: Examples include azathioprine, cyclosporine, dupilumab, methotrexate, and upadacitinib.
Ultraviolet (UV) light therapy: Effective for widespread AD.
Alitretinoin: Specifically approved for severe chronic hand AD in adults.
Oral corticosteroids are not recommended for routine use in AD due to significant side effects and the risk of rebound flares upon discontinuation. Dermatologist referral is advised for patients requiring systemic therapy.
Flare Prevention
Preventing flares is a cornerstone of AD management and involves routine application of moisturizers at least once daily. Long-term intermittent use of topical corticosteroids or calcineurin inhibitors on previously affected areas (e.g., twice weekly) may also help maintain remission. Tacrolimus is approved in Canada for this purpose, while other regimens are considered off-label. Early use of calcineurin inhibitors at the onset of a flare may prevent progression.
Management of Secondary Infection
Secondary bacterial infections in AD may present as oozing, crusting, or bright red friable skin. Localized infections can be managed with topical antibiotics, while systemic antibiotics may be necessary for widespread infection or systemic symptoms. The use of prophylactic antibiotics or antiseptics (e.g., bleach baths) for recurrent infections has inconsistent evidence, with studies showing mixed results on their effectiveness.
Sleep Disturbance
Sleep disturbance, often due to itching, is a common issue in poorly controlled AD. Effective disease management is the most critical factor in improving sleep. Sedating antihistamines (e.g., diphenhydramine, hydroxyzine) may provide short-term relief for sleep disturbances, although their efficacy in managing AD is limited. Non-sedating antihistamines have little effect on pruritus in AD.
AD Management in Pregnancy and Breastfeeding
During Pregnancy
AD often worsens during pregnancy, with most cases occurring in the first two trimesters.
Nonpharmacologic strategies like moisturizers and avoiding irritants should be maximized.
Topical corticosteroids are preferred (low- to mid-potency), while systemic agents like cyclosporine or azathioprine are reserved for severe cases under close monitoring.
Methotrexate and upadacitinib are contraindicated during pregnancy, while dupilumab appears to have minimal teratogenic risk based on limited human data.
During Breastfeeding
Moisturizers and topical corticosteroids remain the primary treatments. Potent corticosteroids should be used sparingly to minimize systemic absorption.
Topical calcineurin inhibitors are second-line options and appear to have minimal absorption into breast milk. Avoid applying these agents to the nipple or areola to prevent infant ingestion.
UVB therapy is considered safe during breastfeeding, while systemic agents like methotrexate, cyclosporine, and upadacitinib should be avoided.
Therapeutic Tips
Topical Vehicle Selection: Ointments are highly effective for AD but may have lower patient adherence due to their greasy texture.
Education: Patients should understand that AD is a chronic, relapsing condition that can be controlled but not cured.
Trigger Avoidance: Heat, stress, and sweating often exacerbate itching and should be minimized where possible.
Refractory Lesions: Resistant patches of dermatitis may require short-term treatment with higher-potency corticosteroids.
Histamine Blockade: Pruritus in AD is not primarily mediated by histamine, so non-sedating antihistamines are generally ineffective, though they may alleviate allergic symptoms.
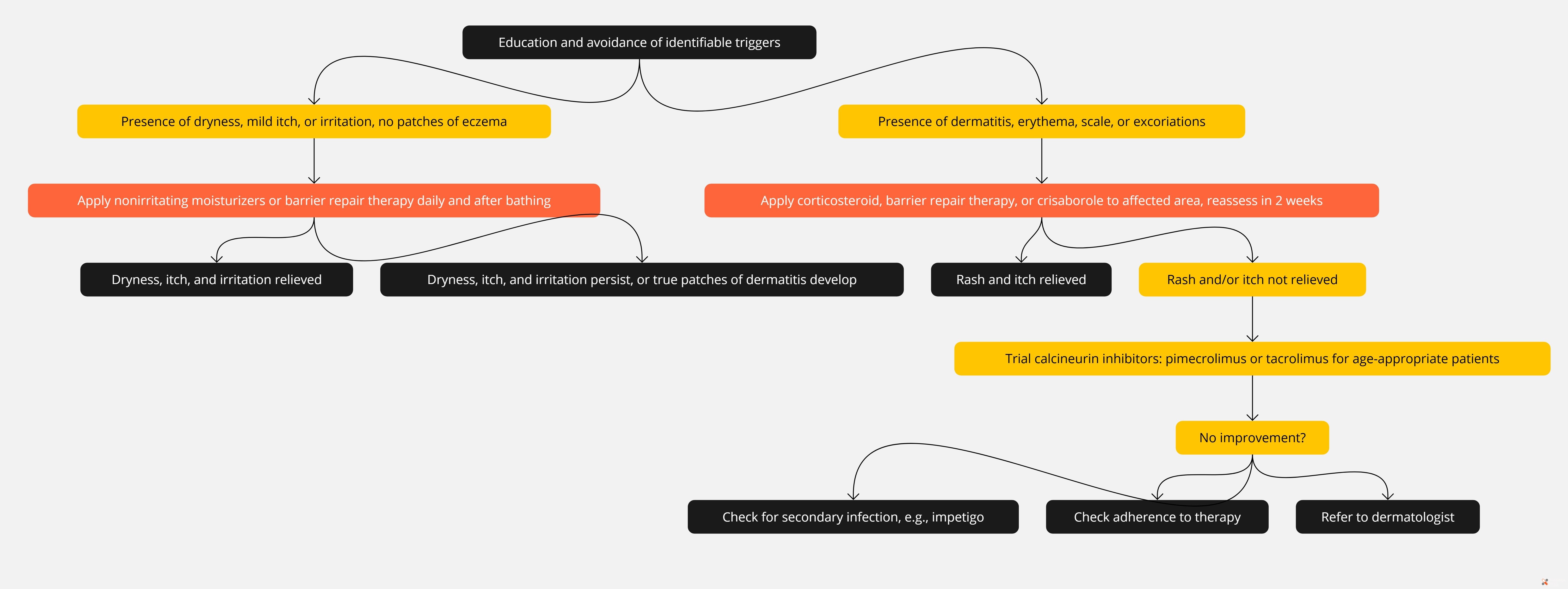
Algorithms for Atopic Dermatitis