Introduction
This chapter is designed for the PEBC preparation exam and focuses on Attention-Deficit Hyperactivity Disorder (ADHD), a widely recognized neurodevelopmental disorder in children. ADHD affects approximately 4–12% of school-aged children in North America and 2–8% of preschoolers aged 3 to 5 years. The condition is primarily characterized by three main symptoms: inattention, hyperactivity, and impulsivity. These behaviors are significantly more pronounced than what is typically expected for a child's age or developmental stage, often leading to disruptions in their growth and daily functioning.
Key Features of ADHD
Impact Across Settings: ADHD symptoms appear in at least two different environments, such as home, school, or work.
Types of ADHD: Individuals may be classified into one of three categories:
Primarily Inattentive Subtype
Primarily Hyperactive/Impulsive Subtype
Combined Subtype (most common)
Effects: The disorder negatively impacts academic performance, social relationships, and cognitive abilities.
Refer to Table 1 for a detailed list of ADHD symptoms and diagnostic criteria.
Onset and Lifespan Considerations
ADHD symptoms usually begin before age 12 and can persist into adulthood. Although the DSM-5-TR specifies symptom onset before age 12, recent research suggests that ADHD can develop in young adults with no childhood diagnosis. Approximately 3–4% of adults live with ADHD.
Comorbid Conditions
Children and adults with ADHD often face additional mental health challenges, including:
Oppositional Defiant Disorder (ODD)
Learning Disabilities
Mood and Anxiety Disorders
Substance Use Disorders
This foundational knowledge is critical for pharmacy professionals preparing for the PEBC exams. Understanding ADHD’s characteristics, diagnostic criteria, and associated conditions will aid in addressing patient care and medication management in clinical settings.
Criteria for ADHD Diagnosis:
Consistent Pattern of Inattention and/or Hyperactivity-Impulsivity that Disrupts Normal Activities and Development, as shown by (1) and/or (2).
Some symptoms of inattention or hyperactivity-impulsivity appeared before age 12.
Symptoms are present in two or more settings (e.g., home, school, work, or with friends).
There is clear evidence these symptoms negatively impact social, academic, or work-related functioning.
Symptoms are not due to another mental disorder (e.g., mood disorder, anxiety disorder, or substance use).
Therapy Goals for ADHD Management
Reduce ADHD Symptoms: Aim to eliminate or significantly reduce symptoms to improve daily functioning.
Enhance Performance: Focus on improving behavioral, academic, and workplace performance.
Boost Self-Esteem and Social Skills: Help patients build confidence and improve relationships with family, peers, and colleagues.
Prevent Complications: Minimize the risk of associated issues such as mood disorders, anxiety, or substance use disorders.
Minimize Medication Side Effects: Ensure that treatment is effective while limiting adverse effects.
Improve Quality of Life: Support overall well-being and life satisfaction.
Diagnostic Approach for ADHD
Currently, there are no lab tests or imaging studies to confirm ADHD. Diagnosis relies on identifying behavioral patterns consistent with ADHD diagnostic criteria.
Steps in the Diagnostic Process
Behavioral Criteria:
Identify 6 or more symptoms in children or 5 or more symptoms in individuals aged 17 and older, lasting for at least 6 months.
Symptoms must be inconsistent with developmental norms and significantly impact daily life (see Table 1 for details).
Gather Comprehensive Information:
Collect input from the patient, caregivers, teachers, and psychologists (if involved) to assess:
Symptom severity and duration.
Impact on social, academic, or occupational functioning.
Age of symptom onset.
Interactions with family and peers.
Triggers or situations that worsen or improve symptoms.
Possible comorbid conditions, such as oppositional defiant disorder (ODD), mood/anxiety disorders, tic disorders, or learning disabilities.
Evaluate for Substance Use Disorders:
In some cases, urine drug screening may be recommended before starting stimulant medications and periodically during treatment.
Use Rating Scales:
Leverage tools like the CADDRA Assessment Toolkit to track symptoms and treatment progress.
Notable tools include the SNAP-IV Teacher and Parent Rating Scale, which is particularly valuable for feedback from parents and educators.
Review Medical and Developmental History:
Obtain birth/prenatal history, noting premature birth or in utero exposure to substances.
Conduct a physical examination to assess hearing, vision, thyroid function, neurological status, and cardiac health.
Screen for conditions like anemia or syndromes such as Down syndrome.
Cardiovascular Screening Before Stimulants:
Obtain baseline blood pressure, heart rate, height, and weight, and reassess during follow-up visits.
Routine ECGs are not recommended for children without a history of heart disease or abnormal physical findings.
Consider ECGs or cardiology consultation for patients with:
Known cardiac abnormalities.
Family history of heart disease or sudden cardiac death.
Abnormal findings during a physical exam (e.g., elevated BP or irregular heart rate).
Therapeutic Approaches for ADHD Management
Managing ADHD requires a structured, multimodal approach that combines behavioral interventions, educational support, and pharmacological treatments tailored to the individual's age, symptom severity, and family preferences. Below is a detailed discussion of the therapeutic choices available.
Multimodal Treatment: The Gold Standard
For both children and adults, combining nonpharmacologic and pharmacologic therapies is considered the most effective strategy for managing ADHD. Key considerations include:
Preschool-Aged Children (3–5 years):
First-Line: Behavioral interventions, such as parent and teacher training, are recommended as the initial treatment.
Pharmacologic Therapy: Medications like methylphenidate may be introduced for moderate to severe ADHD if behavioral therapy alone is insufficient. However, this should only occur when the benefits outweigh potential risks due to limited long-term data in this age group.
Shared-Care Approach:
Involve caregivers and patients in treatment planning, taking their values and preferences into account.
Recognize the chronic nature of ADHD and its frequent association with psychiatric and developmental comorbidities.
Nonpharmacologic Treatment Options
Nonpharmacologic therapies focus on modifying behaviors and improving social, emotional, and academic functioning. While these therapies are less effective than stimulants at reducing ADHD core symptoms, they play an essential role in comprehensive care.
Behavioral Interventions
Behavioral Therapy: Trains parents and teachers to manage ADHD symptoms by reinforcing positive behaviors and reducing negative ones. These therapies improve:
Social interactions
Family dynamics
Self-esteem
ADHD-associated behaviors
Sleep Hygiene: Incorporating sleep-focused strategies into behavioral interventions reduces ADHD symptoms and improves sleep quality at 3–6 months post-intervention.
Cognitive and Social Skills Training
Parent Training: Equips parents with skills to manage ADHD-related challenges, boosting their confidence and reducing stress.
Mindfulness and Social Skills Training: Helps patients develop self-regulation and improve relationships.
Exercise and Lifestyle Adjustments
Exercise: Aerobic activities and yoga have been shown to reduce ADHD symptoms, improve cognitive function, and decrease anxiety.
Dietary Changes: Some evidence suggests that eliminating certain sugars, dyes, or preservatives may reduce hyperactivity in some children. However, robust evidence is lacking, and no specific dietary recommendations can be made.
Pharmacologic Treatment Options
Medications are typically reserved for individuals with a clear ADHD diagnosis and significant impairments in learning, social interactions, or behavior. Stimulants are the first-line treatment for ADHD core symptoms (hyperactivity, impulsivity, and inattention).
Stimulants
First-Line Stimulants: Long-acting formulations such as:
Lisdexamfetamine (Vyvanse)
Methylphenidate extended-release (Concerta, Biphentin)
Mixed amphetamine salts (Adderall XR)
These medications have proven efficacy in patients aged 6 years and older, with at least 70% showing a significant reduction in symptoms. Advantages include:
Once-daily dosing
Better adherence
Reduced need for school-time medication administration
Lower risk of rebound hyperactivity
Second-Line Stimulants: Intermediate-release formulations like Ritalin SR and Dexedrine Spansules are used when flexible dosing is required. They may also serve as add-ons to long-acting formulations.
Immediate-Release Stimulants: Used for short-term symptom management or as adjunct therapy in specific cases.
Non-Stimulant Medications
Atomoxetine (Strattera):
A norepinephrine reuptake inhibitor, recommended for patients who do not respond to or cannot tolerate stimulants.
Takes 3–4 weeks to show effects; effective for those with comorbid anxiety or substance use disorders.
Alpha2-Adrenergic Agonists:
Guanfacine (Intuniv XR): Effective in managing aggression, hyperactivity, and impulsivity, especially in younger children.
Clonidine: Used less frequently due to sedation and hypotension but may be effective in managing tics and sleep issues.
Antidepressants: Considered third-line treatments, beneficial for patients with comorbid depression, anxiety, or tic disorders. Options include:
Bupropion: Moderately effective for both children and adults.
Tricyclic Antidepressants (e.g., Imipramine, Nortriptyline): Less effective than stimulants but may be suitable for patients unable to use first- or second-line therapies.
Monitoring and Safety Considerations
Side Effects and Risks
Stimulants:
Common side effects: Insomnia, reduced appetite, GI upset, increased heart rate, and blood pressure.
Rare risks: Growth suppression (monitor height/weight every 3–6 months), psychosis, and suicidal ideation.
Cardiovascular risks: Baseline assessments (BP, heart rate, medical history) are essential. Routine ECGs are not required unless cardiac risk factors are present.
Non-Stimulants:
Atomoxetine: Monitor for suicidal thoughts, especially during dose changes.
Alpha2-Agonists: Watch for sedation and hypotension.
Long-Term Monitoring: Use standardized rating scales (e.g., SNAP-IV) to evaluate progress and side effects across home and school environments.
Substance Abuse and Diversion
Educate patients and families about the risks of medication misuse.
Monitor for signs of substance use, such as insomnia, irritability, or frequent requests for early refills.
Consider non-stimulant options for patients at higher risk of substance abuse.
Therapeutic Approaches for ADHD Management
Managing Common Side Effects of ADHD Treatments
Managing the side effects of ADHD treatments is essential to ensure patient safety and adherence to therapy. Below is an organized and detailed explanation of strategies to monitor and address common adverse effects associated with ADHD medications.
1. Appetite Suppression
Monitoring:
Consistent weight and appetite monitoring is essential. Check for weight changes and signs of appetite suppression every two weeks during the initial phase of treatment, and then every six months.
For children and adolescents, it is equally important to track height regularly to identify potential growth delays.
Management:
Timing of Medication: Administer medications during or after meals to minimize the impact on appetite.
Optimized Nutrition: Encourage high-calorie meals or snacks during periods when appetite is less affected, such as in the evening or early morning before taking the stimulant.
Nutritional Supplements: Consider adding nutritional meal supplements if significant weight loss or insufficient caloric intake occurs.
Alternative Medication Forms: Switch to shorter-acting stimulant formulations to allow appetite to return during parts of the day.
Drug Holidays: Plan medication-free periods, such as weekends or school breaks, to help restore appetite and reduce long-term suppression effects.
Affected Medications:
Stimulants (e.g., methylphenidate, amphetamines)
Atomoxetine
Bupropion
2. Cardiovascular Effects (Elevated Heart Rate and Blood Pressure)
Monitoring:
Regular monitoring of blood pressure (BP) and heart rate (HR) is critical. Assess these parameters within the first two weeks of starting stimulant therapy, and then every three months to track trends over time.
Routine ECGs are typically not required for patients without a history of cardiovascular issues. However, consider ECG monitoring for individuals with known risk factors or a history of cardiac abnormalities.
Management:
Discontinue and Consult: If significant cardiovascular changes are noted—such as sustained high BP (above the 95th percentile for age), persistent tachycardia, or arrhythmias—discontinue the medication and consult a cardiologist.
Medication Selection: For patients with underlying cardiac risks, consider alternative treatments such as alpha-2 agonists (e.g., guanfacine, clonidine) or non-stimulant options.
Affected Medications:
Stimulants: Can cause increased BP and HR.
Alpha-2 Agonists: Can decrease BP/HR but should be tapered gradually to avoid rebound hypertension.
Tricyclic Antidepressants (TCAs): May cause tachycardia and other cardiovascular effects.
3. Psychiatric Effects (Anxiety, Irritability, Insomnia, and Tics)
Monitoring:
Track sleep disturbances, anxiety, and other behavioral symptoms weekly during the first month of treatment, and then reassess every three months.
Encourage caregivers to use standardized tools such as the Sleep Disturbance Scale for Children or other sleep habit questionnaires to monitor symptoms at home.
Management:
Initial Adjustment Period: Note that symptoms like anxiety and insomnia often peak during the first 1–2 weeks of therapy and may resolve over time.
Dosing Adjustments: For persistent insomnia, consider adjusting the timing of medication to earlier in the day, switching to a shorter-acting formulation, or adding sedative medications at bedtime (e.g., melatonin or antihistamines).
Lifestyle Modifications: Reduce caffeine intake and minimize stimulating activities, such as screen time or electronic device use, before bedtime to support better sleep hygiene.
Affected Medications:
Stimulants
Atomoxetine
Bupropion
Venlafaxine
Managing ADHD Treatments: Essential Considerations for PEBC Exam Preparation
Drug Holidays
ADHD is often a lifelong condition, but symptoms may decrease during adolescence in some individuals. For patients on ADHD medication, drug holidays provide a valuable opportunity to reassess the need for continued pharmacologic treatment. This approach is particularly relevant for pharmacists preparing for the PEBC exams, as it highlights patient-centered care and evidence-based decision-making.
Annual Drug Holidays: A short break of 2–3 weeks, typically during school or work vacations, allows clinicians to observe ADHD-related behaviors and determine whether medication is still required for the upcoming term.
Extended Breaks: Prolonged drug holidays (e.g., entire summer months) are not recommended for children with moderate to severe ADHD who respond well to medication. The return of disruptive symptoms often outweighs the potential benefits of discontinuation, particularly regarding behavior, social interactions, and self-esteem.
When to Consider Drug Holidays: These may be beneficial in cases of adverse effects, such as growth suppression or significant weight loss (>10% of baseline body weight), or to evaluate the medication's ongoing effectiveness.
Pharmacists must also be aware of withdrawal risks. Abrupt discontinuation of stimulants can cause withdrawal symptoms, particularly in patients on high doses for prolonged periods. Tapering stimulants over several weeks is advised for these patients. Alpha-2 adrenergic agonists, such as clonidine and guanfacine, require gradual tapering (e.g., 0.1 mg/week for clonidine, 1 mg/week for guanfacine) to prevent rebound hypertension. For the PEBC exam, ensure familiarity with these tapering protocols and the rationale behind them.
ADHD Management During Pregnancy and Breastfeeding
Pharmacists must be prepared to counsel patients about managing ADHD during pregnancy and breastfeeding, a topic that may appear in PEBC exam scenarios.
Pregnancy Considerations
ADHD symptoms may worsen during pregnancy due to hormonal changes and psychological stress. The safety of ADHD medications during pregnancy is not well-established, which requires careful evaluation of risks versus benefits:
Nonpharmacologic Management: For mild to moderate symptoms without significant functional impairment, behavioral therapies and other nonpharmacologic approaches are preferred.
Stimulant Use During Pregnancy:
Amphetamines (e.g., amphetamine, dextroamphetamine): Observational data suggest no increased risk of major congenital malformations, making these a safer option.
Methylphenidate: While not associated with overall major malformations, some studies suggest a potential increased risk of cardiac abnormalities, particularly during the first trimester.
Lisdexamfetamine: Insufficient data exist regarding its safety in pregnancy.
Alternative Medications:
TCAs, bupropion, and venlafaxine: Should be used cautiously due to limited efficacy for ADHD.
Atomoxetine: Avoid, especially during the first trimester, due to a lack of data.
Clonidine: Appears safe but has limited data on first-trimester use.
Risperidone and guanfacine: Avoid due to lack of safety data and limited ADHD benefits.
For the PEBC exam, emphasize understanding these medication options, their risks, and nonpharmacologic alternatives during pregnancy.
Breastfeeding Considerations
Pharmacists must also counsel patients on ADHD medication use during breastfeeding, balancing the need for symptom management with the safety of the nursing infant.
Methylphenidate: Minimal transfer into breast milk; infants should be monitored for irritability and poor weight gain.
Amphetamines: Transfer into breast milk; monitor for insomnia, agitation, and weight gain issues in the infant.
TCAs, bupropion, venlafaxine: May be used if effective, with monitoring for sedation and irritability in the infant.
Clonidine and guanfacine: May reduce milk production and cause hypotension in the infant, so alternatives are preferred.
Atomoxetine: Insufficient data; avoid during breastfeeding.
For PEBC exam preparation, focus on identifying medications that are safe for breastfeeding and the appropriate monitoring parameters for nursing infants.
Therapeutic Tips for ADHD Management
Pharmacists preparing for the PEBC exams should be familiar with practical considerations in selecting and monitoring ADHD treatments:
Tailored Medication Selection: Consider the child’s daily schedule, predominant symptoms, adherence likelihood, cost, and risk of side effects.
Crossover Trials: "N of 1" trials comparing stimulant versus placebo or different stimulants can help evaluate therapeutic benefits.
Administration of Long-Acting Stimulants: Educate patients and caregivers on proper administration. Long-acting stimulants should not be crushed or chewed, but some formulations (e.g., Adderall XR, Vyvanse, Biphentin) can be opened and sprinkled on soft foods.
Switching Medications: When transitioning from stimulants to non-stimulants (e.g., atomoxetine) or antidepressants, continue the stimulant at a lower dose while tapering over three weeks to allow the new medication to take effect.
Substance Use Risk: ADHD patients are at higher risk of substance use disorders. Proper treatment with stimulants reduces this risk, a concept that often appears in PEBC exam case studies.
Managing ADHD with Tic Disorders: Stimulants can safely treat ADHD in patients with tic disorders, though they may exacerbate tics in some cases. Alpha-2 adrenergic agonists (e.g., clonidine, guanfacine) can manage both conditions effectively.
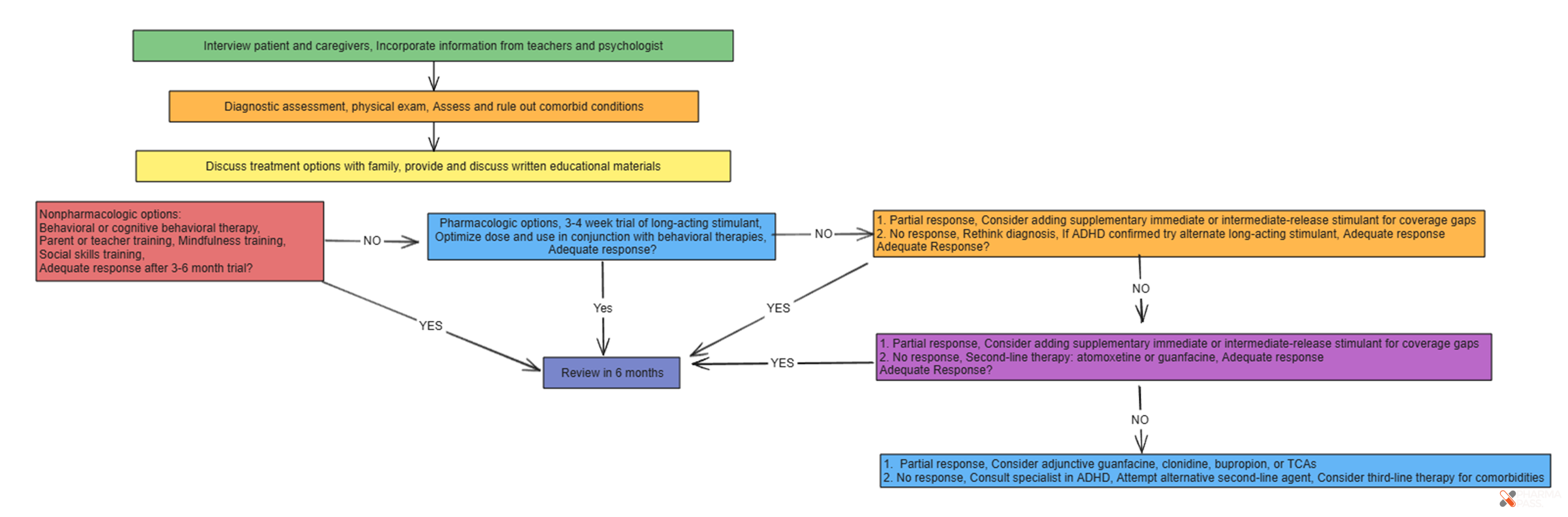
ADHD Algorithm for PEBC exams