| -Introduction |
This chapter serves as a crucial foundation for candidates preparing for the Pharmacy Examining Board of Canada (PEBC) exam, focusing on the autonomic nervous system (ANS) and its interplay with the endocrine system in regulating and integrating bodily functions. The endocrine system communicates with target tissues via changes in blood-borne hormone levels, while the nervous system impacts bodily functions through the rapid transmission of electrical impulses across nerve fibers to effector cells. These cells respond to the release of neuromediator substances, highlighting the intricate mechanisms by which our body maintains homeostasis.
For those studying for the PEBC exam, understanding autonomic drugs—those that achieve their therapeutic effects by either mimicking or modifying ANS functions—is vital. This section lays the groundwork for comprehending the essential physiology of the ANS and the critical role neurotransmitters play in facilitating communication between extracellular events and intracellular chemical changes.
However, it's important for PEBC exam candidates to recognize that while this chapter provides a solid introduction to the ANS and autonomic drugs, the complexity and breadth of these topics may require further exploration beyond this text. Students are highly encouraged to consult external reference books for a more comprehensive understanding of the material. This deeper dive into additional resources will not only bolster your preparation for the PEBC exam but also enhance your grasp of pharmacological principles critical to effective pharmacy practice. Engaging with a broad range of study materials will equip PEBC exam candidates with a robust knowledge base, preparing them for the various scenarios and challenges they may encounter in their professional journey.
What are the main parts of nervous system?
Central Nervous System (CNS): consists of brain and spinal cord. Anything out of that is called PNS
Peripheral nervous system: PNS further is divided into
Afferent: impulses coming into the brain
Efferent: impulses going out of brain that control 2 functions:
Voluntary: Somatic motor nerves (to the skeletal muscles)
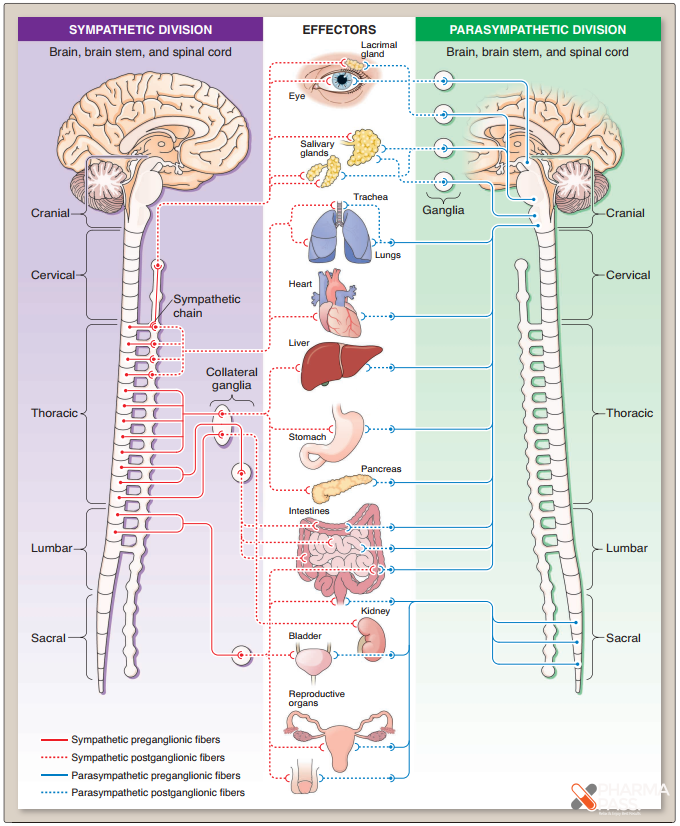
Involuntary: Autonomic nervous system: e.g. intestine, liver, etc. ANS is further divided into 2 sections:
Sympathetic nervous system: fight & flight, used in emergency, fear, stress, etc.
Parasympathetic nervous system: rest & digest, feed & breath, baseline & survival system
What is the autonomic nervous system? It is the involuntary branch of the peripheral nervous system's efferent division.
Please compare sympathetic and parasympathetic nervous system?

Please compare sympathetic & parasympathetic functions?






What are adrenergic receptors (Sympathetic receptors)? Adrenergic receptors, also known as sympathetic receptors, belong to the group of G protein-coupled receptors that interact with the body's naturally produced catecholamines, norepinephrine (noradrenaline) and epinephrine (adrenaline), as well as various medications including β-blockers, β2-agonists, and α2-agonists. These drugs are commonly prescribed for conditions like hypertension and asthma. When catecholamines bind to adrenergic receptors, they typically activate the sympathetic nervous system (SNS), initiating a series of physiological responses.
What are different adrenergic receptors?
What are cholinergic receptors (parasympathetic receptors)? Cholinergic receptors are cell surface proteins that become activated upon binding with the neurotransmitter acetylcholine. These receptors are classified into two categories: nicotinic and muscarinic receptors.
Where is Ach synthesized and released from?Acetylcholine is a crucial neurotransmitter that is released by nerve endings within both the peripheral and central nervous systems. This chemical messenger is produced inside the nerve terminals through the synthesis from choline, which is absorbed from the surrounding tissue fluid into the nerve ending via a specific transport mechanism. In the central nervous system, acetylcholine is involved in various functions including memory and muscle control. In the peripheral nervous system, it is essential for activating muscle actions and influencing the parasympathetic nervous system, which manages bodily functions such as saliva production, digestion, and heart rate.
What are parasympathetic (Cholinergic) receptors?
What are different cholinergic drugs?
What is the difference between catecholamine and non-catecholamine?
non-catecholamines are not substrates for COMT, and some are resistant to MAO degradation.
non-catecholamines are effective orally while most catecholamines are not
1. Septic Shock: Arises when bacteria proliferate in the bloodstream, releasing harmful toxins. Common origins include infections like pneumonia, urinary tract infections, skin infections such as cellulitis, intra-abdominal infections (e.g., a ruptured appendix), and meningitis. Treatment: Medications like Dopamine, Norepinephrine, and Phenylephrine are used, but Dobutamine is typically avoided.
2. Anaphylactic Shock: A severe allergic reaction characterized by hypersensitivity to substances such as insect stings, medications, or foods (like nuts, berries, seafood). Treatment: The primary treatment is Epinephrine.
3. Cardiogenic Shock: Occurs when the heart has been damaged to the point it can no longer pump adequate blood to the body, often following a heart attack or in the context of congestive heart failure. Treatments may include mechanical devices to support heart function and medications such as Dopamine, Norepinephrine, and Dobutamine to improve heart pumping capability.
4. Hypovolemic Shock: Triggered by significant blood and fluid loss, for example, due to traumatic injury, resulting in insufficient blood volume for the heart to pump effectively. Severe anemia can also lead to hypovolemic shock by reducing the blood's oxygen-carrying capacity. Treatment: Management includes administering intravenous (IV) fluids and Dopamine to support blood pressure and volume.
5. Neurogenic Shock: Results from spinal cord injuries, often due to accidents or trauma, affecting the body's ability to control the diameter of blood vessels, leading to low blood pressure. Treatment: Phenylephrine is commonly used to manage this type of shock.
6. Drug-Induced Shock: Shock that occurs as a side effect or reaction to certain medications. Treatment: Treatment often includes Phenylephrine, among other supportive measures.