Introduction to COPD for PEBC exams Preparation
This chapter is designed to equip candidates for the Pharmacy Examining Board of Canada (PEBC) with a comprehensive understanding of Chronic Obstructive Pulmonary Disease (COPD). COPD is a systemic condition predominantly caused by smoking, characterized by progressive yet partially reversible airway limitation and a rising frequency and severity of exacerbations. Importantly, COPD is both preventable and treatable. The hallmark symptoms include shortness of breath and physical activity limitations. Research highlights that genetic variations may influence the manifestation and severity of COPD symptoms, adding complexity to its clinical presentation.
Pathophysiology and Impact of COPD
Individuals with COPD often experience breathlessness, which leads to restricted physical activity. This limitation initiates a vicious cycle of deconditioning, further exacerbating activity restrictions and overall health decline. Smoking cessation and optimal bronchodilation are central to managing COPD, aiming to slow disease progression, alleviate symptoms, and reduce the risk of acute exacerbations. These strategies also help improve or maintain the patient's physical activity levels and quality of life.
Goals of Therapy
The therapeutic objectives in COPD management emphasize slowing disease progression, improving patient comfort, and enhancing quality of life. These goals include:
- Preventing Disease Progression: Through interventions such as smoking cessation and vaccination.
- Relieving Respiratory Symptoms: Optimal bronchodilation to alleviate breathlessness and improve lung function.
- Enhancing Exercise Tolerance: Addressing deconditioning with pulmonary rehabilitation and pharmacotherapy.
- Reducing Exacerbations: Minimizing frequency and severity through prophylactic measures and early treatment of acute episodes.
- Improving Quality of Life: Focusing on physical, psychological, and social well-being.
- Managing Comorbidities: Addressing associated conditions like cardiovascular disease, osteoporosis, and depression.
- Reducing Disability and Mortality: Enhancing functional independence and survival rates.
Diagnostic and Investigative Approach
A systematic evaluation is critical for diagnosing COPD, assessing severity, and formulating a tailored treatment plan. The diagnostic process involves a combination of clinical history, physical examination, and objective tests.
1. Clinical History
Key elements to evaluate include:
- Symptoms: Chronic cough, sputum production, progressive dyspnea, and activity limitations.
- Triggers and Risk Factors: Tobacco smoking, occupational exposure to dust or chemicals, and air pollution.
- Comorbidities: Conditions such as cardiovascular disease, osteoporosis, or metabolic syndrome.
- Impact on Daily Life: Assessing functional and psychological limitations.
- Past Exacerbations: Frequency, severity, and treatment history.
2. Physical Examination
While relatively insensitive for diagnosis, it can reveal:
- Early Signs: Dyspnea and wheezing.
- Advanced Findings: Hyperinflation, hypoxemia, or signs of pulmonary hypertension.
3. Objective Measurements
- Spirometry: The gold standard for COPD diagnosis, requiring a post-bronchodilator FEV1/FVC ratio of less than 0.7 or below the Lower Limit of Normal (LLN).
- Additional Tests:
- Lung volume and diffusion capacity assessments.
- CBC for polycythemia or anemia.
- Chest X-ray to exclude other conditions like malignancy or bronchiectasis.
- Pulse oximetry and arterial blood gases in severe cases.
- Alpha1-antitrypsin levels in patients with atypical presentations or a family history of COPD.
- Eosinophil counts for asthma-COPD overlap syndrome (ACOS).
4. Severity Assessment Tools
Two commonly used scales help evaluate symptom burden and track disease progression:
- Modified Medical Research Council (mMRC) Scale: Grades breathlessness severity based on activity limitations.
- COPD Assessment Test (CAT): A detailed questionnaire to assess COPD’s impact on a patient's life and monitor changes over time.
Table: Modified Medical Research Council (mMRC) Dyspnea Scale
Importance of the mMRC Scale
The mMRC scale is an integral component of COPD assessment and management. It enables healthcare professionals to gauge the severity of dyspnea and its impact on the patient’s daily life, informing therapeutic decisions. For the PEBC exams, understanding the scale and its application is critical for accurate patient evaluations and evidence-based care planning.
Pharmacologic and Nonpharmacologic COPD Management
Short-Acting Bronchodilators (SABAs and SAMAs)
Role of Short-Acting Beta2-Agonists (SABAs):
- Indications: Recommended as PRN (as needed) therapy across all COPD severity stages for immediate symptom relief.
- Common Agents: Salbutamol (e.g., Ventolin, Airomir) and Terbutaline (e.g., Bricanyl DPI).
- Pharmacology: SABAs have a rapid onset and a duration of action of 4–6 hours. Doses can be adjusted (doubled or tripled) for better bronchodilation, though side effects like tachycardia, tremors, and hypokalemia should be monitored.
Role of Short-Acting Muscarinic Antagonists (SAMAs):
- Common Agent: Ipratropium (Atrovent).
- Comparison with SABAs: Slower onset but longer duration of action (up to 8 hours).
- Dosing: Standard dose is 40 mcg 3–4 times daily, with the potential for dose doubling or tripling without significant side effects.
Combination Therapy with SABA and SAMA:
- Combination Products: Ipratropium/Salbutamol (Combivent Respimat).
- Benefits: Provides greater and more sustained bronchodilation compared to monotherapy, along with fewer side effects and improved lung function.
Oral Beta2-Agonists:
- Role: Not recommended for routine COPD management due to limited advantages and higher side effect risks.
Long-Acting Bronchodilators (LAMAs and LABAs)
Long-Acting Muscarinic Antagonists (LAMAs):
- First-Line Agent: Tiotropium (Spiriva DPI or Respimat).
- Benefits: Decreases exacerbations, reduces hospitalizations, and improves dyspnea and quality of life.
- Dosage: Once-daily inhalation; 18 mcg via DPI or two 2.5 mcg inhalations via SMI.
- Safety: No increased cardiovascular risk noted.
- Other Agents:
- Glycopyrronium (Seebri Breezhaler): Faster onset, once-daily dosing.
- Aclidinium (Tudorza Genuair): Twice-daily dosing, comparable efficacy to tiotropium.
- Umeclidinium (Incruse Ellipta): Once-daily dosing with evidence of reduced moderate exacerbations.
- First-Line Agent: Tiotropium (Spiriva DPI or Respimat).
Long-Acting Beta2-Agonists (LABAs):
- Common Agents: Salmeterol (Serevent Diskus) and Formoterol (Oxeze Turbuhaler).
- Formoterol: Advantage of rapid onset (<3 minutes) compared to salmeterol.
- Ultra-Long-Acting Agents:
- Indacaterol (Onbrez Breezhaler): Rapid onset and once-daily dosing; comparable to tiotropium in efficacy.
- Olodaterol: Available in combination with LAMAs; effective for improving lung function and exercise capacity.
- Common Agents: Salmeterol (Serevent Diskus) and Formoterol (Oxeze Turbuhaler).
LAMAs vs. LABAs:
- LAMAs have a stronger effect on reducing exacerbations and hospitalizations compared to LABAs.
Combination Therapy (LAMA/LABA):
- Indications: For patients with persistent symptoms despite monotherapy or frequent exacerbations.
- Products: Include glycopyrronium/indacaterol (Ultibro Breezhaler) and umeclidinium/vilanterol (Anoro Ellipta).
- Benefits: Provides superior bronchodilation, symptom relief, and exacerbation reduction compared to monotherapy.
Combination Inhaled Corticosteroids and Long-Acting Bronchodilators
ICS/LABA Combinations:
- Indications: For patients with moderate to severe COPD and frequent exacerbations.
- Products: Examples include fluticasone/salmeterol (Advair Diskus) and budesonide/formoterol (Symbicort Turbuhaler).
- Risks: Increased risk of pneumonia, especially with fluticasone. Budesonide may have a slightly lower risk.
- Overlap with Asthma: ICS/LABA combinations are particularly beneficial in COPD with overlapping asthma symptoms.
Triple Therapy (ICS/LAMA/LABA):
- Indications: Reserved for patients with repeated exacerbations (≥2 per year or ≥1 requiring hospitalization).
- Benefits: Reduces exacerbation frequency, improves lung function, and enhances quality of life.
- Products: Include fluticasone/umeclidinium/vilanterol (Trelegy Ellipta).
- Delivery: Single-inhaler triple therapy (SITT) is preferred to improve adherence.
Additional Therapies
Phosphodiesterase 4 (PDE4) Inhibitors:
- Agent: Roflumilast.
- Indications: Add-on therapy for severe COPD with frequent exacerbations and chronic bronchitis.
- Benefits: Reduces exacerbations and modestly improves lung function.
Methylxanthines:
- Agent: Theophylline.
- Role: Limited due to narrow therapeutic index and significant side effects.
Mucolytics:
- Agent: N-acetylcysteine (NAC).
- Benefits: May reduce exacerbations in moderate to severe COPD patients with frequent exacerbations.
Vitamin D3:
- Indication: Supplementation may benefit COPD patients with low baseline vitamin D levels (<50 nmol/L).
Antibiotics:
- Macrolides (e.g., Azithromycin):
- Reduce exacerbations in patients with frequent exacerbations despite optimal therapy.
- Consider risks like QT prolongation, ototoxicity, and antibiotic resistance.
- Macrolides (e.g., Azithromycin):
Biologics and Immunoglobulin Therapy:
- While studied, these therapies currently lack approval for COPD management.
Nonpharmacologic Measures
Oxygen Therapy:
- Indications: Severe hypoxemia (PaO2 ≤55 mmHg or SaO2 <88%).
- Benefits: Prolongs life when administered for ≥15 hours daily.
Vaccination:
- Influenza Vaccine: Reduces exacerbations and mortality.
- Pneumococcal Vaccine: Recommended for all COPD patients to reduce pneumonia risk.
- COVID-19 Vaccine: Essential for reducing complications in COPD patients.
Delivery Systems and Adherence
Inhaler Types:
- Devices include pMDIs, DPIs, SMIs, and nebulizers.
- Patient Education: Correct inhaler technique is critical for optimal drug delivery.
Adherence:
- Challenges: Long-term adherence is poor but improves with simpler dosing regimens (e.g., once-daily therapy).
- Strategies: Use of single-inhaler combinations enhances compliance.
Treatment of Acute Exacerbations of COPD (AECOPD)
Acute exacerbations of COPD (AECOPD) are episodes of worsening respiratory symptoms, including dyspnea, sputum volume, and sputum purulence. These episodes accelerate lung function decline and lead to increased healthcare utilization, including hospitalizations. The strongest predictor of future exacerbations and mortality is a history of prior exacerbations, making it crucial to identify and treat frequent exacerbators promptly.
Contributing Factors and Prevention
Triggers:
- Acute respiratory infections (viral and bacterial) account for two-thirds of exacerbations.
- Non-infectious causes include exposure to air pollution and cold weather.
- Common factors associated with exacerbations include female gender, advanced age, low FEV1, multiple comorbidities, and low physical activity levels.
Preventive Measures:
- Ensure appropriate immunization (e.g., influenza and pneumococcal vaccines).
- Optimize baseline symptom control through effective bronchodilation and nonpharmacologic measures.
- Develop and educate patients on personalized COPD action plans.
Systemic Corticosteroids
- Role: Oral corticosteroids help shorten exacerbation duration, improve lung function, and reduce hospital stays.
- Standard Therapy:
- Dose: Prednisone 30–40 mg orally daily for 5 days.
- Tapering: Not necessary for short courses lasting ≤2 weeks.
- Timing: Administration within 30 days of an acute exacerbation reduces the risk of recurrence. Therapy beyond 30 days is not recommended.
Antibiotics
Indications:
- Antibiotics are warranted in patients presenting with at least two of the following cardinal symptoms:
- Increased sputum purulence
- Increased sputum volume
- Worsening dyspnea
- Also indicated for patients requiring mechanical ventilation or those at high risk for poor outcomes (e.g., ≥4 exacerbations in the previous year).
- Antibiotics are warranted in patients presenting with at least two of the following cardinal symptoms:
Common Pathogens:
- Uncomplicated cases: Haemophilus influenzae, Moraxella catarrhalis, Streptococcus pneumoniae.
- Complicated cases (e.g., ≥4 exacerbations/year): Add Enterobacteriaceae and Pseudomonas aeruginosa.
Empiric Antibiotic Selection:
- Tailor choice based on risk factors, local resistance patterns, and previous antibiotic use. Re-evaluate patients not responding within 24–36 hours.


Clinical Insights for PEBC Exam Preparation
- Understand when to initiate systemic corticosteroids and antibiotics based on patient presentation.
- Tailor empiric antibiotic therapy to patient risk factors and microbial susceptibility.
- Recognize the importance of oxygen therapy in managing hypoxemia while avoiding complications.
- Emphasize preventive strategies, including vaccination and optimized baseline symptom management, to reduce AECOPD risks.
Algorithm: Pharmacologic Management of COPD
1. Address Risk Factors
- Encourage smoking cessation.
- Promote pneumococcal and annual influenza vaccination.
- Minimize exposure to occupational and environmental irritants.
2. Initiate Self-Management
- Develop and provide a written COPD action plan.
- Educate patients on recognizing exacerbation warning signs and initiating appropriate measures.
3. Encourage Physical Activity
- Enroll patients in activity and exercise programs, such as pulmonary rehabilitation or local senior/cardiac programs.
4. Initiate Bronchodilators and Provide Education
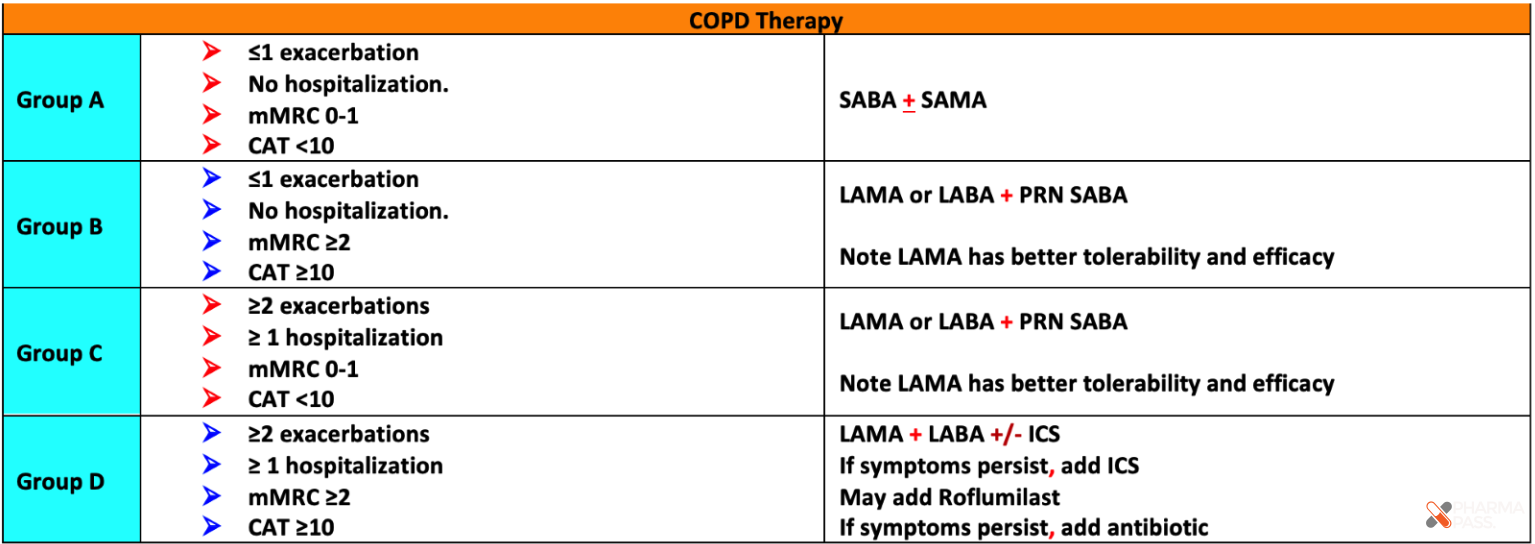
- For All COPD Patients (Mild Cases, CAT < 10, mMRC 0–1):
- Initiate Short-Acting Beta2-Agonist (SABA) as needed (PRN).
- For Moderate to Severe COPD (CAT ≥ 10, mMRC ≥ 2):
- Infrequent Exacerbators: Start with LAMA or LABA.
- Frequent Exacerbators: Use LAMA/LABA combination therapy.
- Provide inhaler technique education and assess adherence at follow-up visits.
5. Step-Up or Step-Down Therapy
- LAMA or LABA → escalate to LAMA/LABA as needed.
- If further exacerbations persist:
- Add ICS to create LAMA + ICS/LABA or ICS/LAMA/LABA triple therapy.
6. Initiate Pulmonary Rehabilitation
- Recommended for patients with persistent symptoms and/or exacerbations despite triple therapy.
7. Add Oral Therapies (if necessary)
- Include options such as:
- Phosphodiesterase-4 (PDE4) inhibitors.
- Macrolides for prophylaxis.
- Mucolytics in selected cases.
8. Add Oxygen Therapy
- Indicated for patients with severe resting hypoxemia (PaO2 ≤ 55 mmHg or SaO2 < 88%).
9. Consider Surgical Options
- For advanced COPD cases, assess the need for:
- Lung volume reduction surgery.
- Lung transplantation.