Introduction to Pediatric Constipation for PEBC Exam Preparation
Preparation Note This chapter is specifically tailored for the PEBC (Pharmacy Examining Board of Canada) exams, ensuring comprehensive coverage of pediatric constipation to enhance clinical knowledge and exam readiness.
Constipation is a prevalent concern in pediatric healthcare, affecting approximately 9.5% of children from infancy to adolescence (0-18 years). This condition is particularly common during key developmental stages, such as toilet training in infants and young children.
Classification and Diagnosis Most cases of constipation in children are classified as functional, meaning they are not linked to underlying medical conditions like anatomical abnormalities. Functional constipation is diagnosed using the Rome IV criteria, which provide a structured framework for assessment (see Table 1 and Table 2). A thorough patient history and physical examination are essential to rule out rare but significant organic causes. Extensive diagnostic investigations are generally unnecessary unless red flags are identified.
Key Contributing Factors The primary driver of pediatric constipation is stool withholding, often due to the pain associated with passing hard stools. Additional contributing factors include:
Diet and Hydration: Low fiber intake and inadequate fluid consumption.
Dietary Transitions: Introduction of solid foods, switching from breast milk to formula, or transitioning to whole milk.
Behavioral Factors: Children may avoid defecation due to discomfort, leading to worsening symptoms.
Gender Differences: While constipation affects both genders, males are more prone to encopresis (fecal incontinence) once they are no longer using diapers.
Impact on Quality of Life Constipation can significantly diminish the quality of life for both children and their families. It can negatively impact physical health, emotional well-being, and social interactions. Additionally, it often results in increased healthcare visits and resource utilization.
Diagnostic Criteria
Table 1: Rome IV Diagnostic Criteria for Functional Constipation in Neonates/Toddlers Neonates and toddlers refer to children from birth to 4 years of age.
Table 2: Rome IV Diagnostic Criteria for Functional Constipation in Children/Adolescents Children and adolescents refer to individuals aged 4 to 18 years.
Goals of Therapy for Pediatric Constipation
Establish Regular Bowel Movements: Achieve consistent, soft, and pain-free bowel movements.
Interrupt Withholding Behaviors: Address both voluntary and involuntary stool withholding to reduce retention.
Normalize Rectal Size: Decrease rectal distention to restore normal rectal girth.
Restore Sensation and Urge: Re-establish the natural sensation and reflex to defecate.
Achieving these therapeutic goals can be a prolonged process, often taking several months to years. Relapses are frequent and require ongoing monitoring and management.
Assessment of Pediatric Constipation
Onset and Duration: When constipation began and how long symptoms have persisted.
Bowel Movement Frequency: Number of bowel movements per week.
Stool Characteristics: Size, shape, and consistency of stools.
Abdominal Pain: Presence of discomfort, cramping, or generalized pain.
Pain During Defecation: Any reports of painful bowel movements.
Withholding Behaviors: Posturing or other signs of stool retention.
Fecal Incontinence: Incidents of stool leakage in toilet-trained children.
Stool Frequency in Infants:
Breastfed Infants: Stool frequency may decrease from 6 times/day to 2–3 times/day after the first three months.
Formula-fed Infants: Less fluctuation, averaging 1-2 bowel movements daily.
Breastfed Infants with Longer Intervals: Extended intervals between bowel movements are normal and typically do not require intervention unless distress is present.
Abdominal Pain: Often the primary complaint, sometimes overshadowing stool-related symptoms.
Fecal Incontinence/Encopresis: Hard stool accumulation can lead to overflow incontinence, manifesting as frequent small bowel movements or diarrhea.
Abdominal Examination: Palpable fullness or fecal mass, particularly in the left lower quadrant.
Perianal/Low Back Examination: Presence of anal fissures, which may cause pain and minor rectal bleeding.
Rectal Examination: Confirms fecal impaction but may not be required if diagnosis is evident from history.
Radiography (X-ray): Limited use; may assist when physical examination is inconclusive. Over-reliance should be avoided.
Thyroid-Stimulating Hormone (TSH): Performed if hypothyroidism symptoms are present.
Tissue Transglutaminase (tTG): May be considered if celiac disease is suspected but not routinely recommended.
🚩Red Flag
Early Onset: Constipation beginning within the first month of life
Delayed Meconium Passage: Meconium passed more than 48 hours after birth.
Ribbon-Like Stools: Narrow or ribbon-shaped stools.
Unexplained Rectal Bleeding: Blood in stools without evidence of anal fissures.
Growth Concerns: Poor growth or failure to thrive.
Abdominal Distention: Severe bloating or distended abdomen.
Perianal and Lower Back Issues:
Abnormal anal positioning.
Reduced muscle tone or reflexes in the lower extremities.
Presence of sacral dimples or hair tufts along the spine.
Deviation in the gluteal cleft.
Rectal Examination:
Explosive stool release following digital rectal examination.
Nonpharmacologic Approaches
Education and Awareness: Explain the nature of constipation to parents and children. Address the child’s lack of awareness regarding stool retention and fecal incontinence. Stress that constipation is common and can be managed.
Hydration and Diet: Encourage adequate fluid intake and a balanced diet rich in fiber. The recommended fiber intake can be calculated by adding 5 g to the child’s age in years.
Physical Activity: Promote daily physical activity to enhance bowel function.
Toilet Training and Routine: Establish regular toilet schedules, encouraging the child to sit for up to 5 minutes about 30 minutes after meals to harness the gastrocolic reflex. Use footstools to support proper posture.
Positive Reinforcement: Use reward charts to encourage toilet use. Avoid reprimanding or punishing the child.
Behavior Monitoring: Track stool patterns and withholding behaviors. A stool journal or the Bristol Stool Form Scale can help document progress.
Dietary Adjustments: Trial elimination of cow’s milk proteins for 2–4 weeks in cases of persistent constipation.
Natural Remedies: Use juices like pear, prune, or apple to ease mild constipation.
Pharmacologic Management
Osmotic Laxatives: Polyethylene glycol 3350 (PEG 3350) is the first-line agent for both clean-out and maintenance phases. High doses (1.5 g/kg/day) are effective for fecal impaction and offer convenience with minimal discomfort. Evacuation typically occurs within 24–48 hours.
Maintenance Therapy: PEG 3350 is preferred over lactulose, as it produces fewer side effects like bloating. Lactulose may be used if PEG 3350 is unavailable. Mineral oil is less effective and not recommended for infants or children at risk of aspiration.
Stimulant Laxatives: Senna or bisacodyl can be used if there is no stool passage after 3 days of osmotic therapy. Concerns about dependency are minimal when used as needed.
Alternative Agents: Newer agents like prucalopride and lubiprostone have limited roles in pediatric constipation.
Rectal Interventions: Glycerin suppositories provide rapid relief, particularly for infants. Sodium phosphate enemas are another option but should be used sparingly due to invasiveness.
Treatment Duration and Relapse Management
Treatment typically spans several months. Full symptom resolution should be maintained for at least 1 month before tapering therapy.
Relapses are common and may result from dietary changes, school routines, travel, or emotional stress. Clean-out therapy may need to be repeated in cases of relapse.
Risk Factors for Relapse or Delayed Response
Male gender.
Constipation onset before age 1.
Presence of encopresis.
ADHD or neurodevelopmental disorders.
History of trauma or adverse childhood experiences.
Therapeutic Notes
Adjust laxative doses to achieve soft stools without leakage. PEG 3350 doses can be titrated higher or lower based on stool consistency.
Use adequate liquid (250 mL per 17 g of PEG 3350) and stir thoroughly to ensure full dissolution.
Encourage routine dosing over as-needed use to avoid fecal incontinence and improve long-term outcomes.
Minimize rectal interventions to avoid reinforcing withholding behaviors.
Foster a supportive environment—parental encouragement and understanding play a vital role in treatment success.
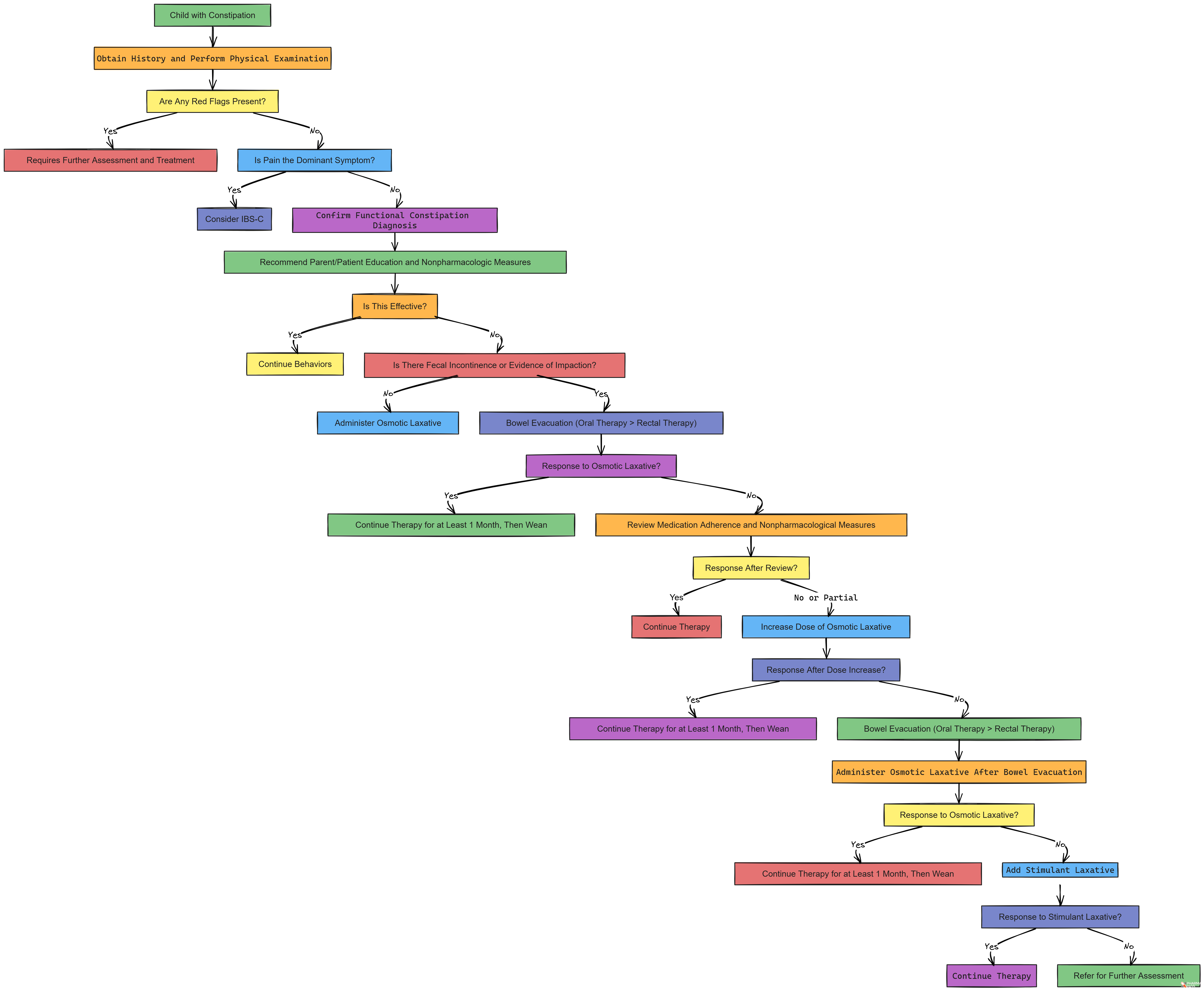
Pediatric Constipation Management Algorithm
Child with Constipation
⬇️Obtain History and Perform Physical Examination
⬇️Are Any Red Flags Present (See Table 3)?
Yes → Requires Further Assessment and Treatment
No → Proceed to Step 4
⬇️Is Pain the Dominant Symptom?
Yes → Consider IBS-Ca (Irritable Bowel Syndrome with Constipation)
No → Confirm Functional Constipation Diagnosis
⬇️Recommend Parent/Patient Education and Nonpharmacologic Measures:
Schedule Sitting
Avoid Withholding
Increase Fluid Intake
Increase Fibre
Follow a Healthy Diet
⬇️Is This Effective?
Yes → Continue Behaviors
No → Proceed to Step 7
⬇️Is There Fecal Incontinence or Evidence of Impaction?
No → Administer Osmotic Laxative
Yes → Bowel Evacuation (Oral Therapy Preferred Over Rectal Therapy)
⬇️Response to Osmotic Laxative?
Yes → Continue Therapy for at Least 1 Month, Then Wean
No → Review Medication Adherence and Nonpharmacological Measures
⬇️Response After Review?
Yes → Continue Therapy
No or Partial → Increase Dose of Osmotic Laxative
⬇️Response After Dose Increases?
Yes → Continue Therapy for at Least 1 Month, Then Wean
No → Bowel Evacuation (Oral Therapy > Rectal Therapy)
⬇️Administer Osmotic Laxative After Bowel Evacuation
⬇️Response to Osmotic Laxative?
Yes → Continue Therapy for at Least 1 Month, Then Wean
No → Add Stimulant Laxative
⬇️Response to Stimulant Laxative?
Yes → Continue Therapy
No → Refer for Further Assessment
Downnload the Full Size Algorithm From Here